↧
Post Cataract & Post Refractive Ophthalmic Products
↧
home high light 1
 some content here for #1
some content here for #1
↧
↧
ISO Certificate

↧
SolarShield® Post Cataract Sunglasses
|
 |

Click to Enlarge |
SolarShield® Post Cataract Sunglasses
|
 |

|
| All include Black drawstring case | ||
 29009A YELLOW |
 29010 CLEAR |
 29008A AMBER |
↧
Encore® Moisture Retention Eyeshield
Designed to help reduce symptoms associated with Dry Eye

5822MS – Encore® Clear. Click to Enlarge. |
|
↧
↧
Reminder to Check Provita Smokehood Expiration Dates
Dear Tecfen Customers and Friends,
For all Provita Smoke Hood owners, please take some time to check the expiration date on those you have in use. There is a four year shelf life on all hoods, and the expiration date can be found labeled on the front of the smokehood package.
The Provita Smoke Hood is a personal escape hood that provides protection from the effects of most toxic smoke fumes, allowing the wearer vital minutes to calmly evacuate a dangerous smoke filled environment. For use in aviation, marine and ground transportation, as well as high rise buildings.
Please let us know if you need to place an order for smoke hoods, or if you have any additional questions.

↧
The long and short of corneal preservation times
by Maxine Lipner EyeWorld Senior Contributing Writer
Studying graft success in tissue that was preserved up to 14 days

The long and short of corneal preservation times
Just how long can corneal tissue be kept and still remain viable for use? Investigators determined that tissue stored for up to 11 days had success rates equal to tissue preserved for a much shorter period, according to Jonathan Lass, MD, Case Western Reserve, University Hospitals Eye Institute, Cleveland.
This study, published in JAMA Ophthalmology, grew out of an earlier donor graft study, with investigators deciding that the issue of cornea preservation would be the next major question with regard to the donor pool.(1)
Bias against long storage
“There was a major prejudice against using tissue beyond 7 or 8 days even though the intermediate storage solution was approved by the FDA to go out to 14 days,” Dr. Lass said. “Also, we were aware that the eye banks, because of this prejudice, were shipping the tissue out of the country and successfully using it internationally,” Dr. Lass said. Surgeons in the U.S. were reluctant to use tissue that had been preserved longer, based mainly on what they had been taught. “They learned to do this in their fellowships, but there was no solid evidence for doing this,” he said. Included in the study were 1,330 eyes, with about an equal distribution between both groups, Dr. Lass noted, adding that they chose DSAEK as the procedure with which to test preservation time because this is currently the most common keratoplasty technique in use. In this masked study, the only thing surgeons knew about the donor was the thickness of the corneal tissue after lamellar dissection. “They needed that information for doing the procedure,” Dr. Lass said. When a cornea was found to be eligible, this was then assigned to a patient, with half of the individuals receiving corneas that had been preserved for 7 days or less and the other half preserved for 8–14 days. In addition, the groups were subdivided into 0–4 days, 5–7 days, 8–11 days, and 12–14 days.
Considering findings
At the 3-year mark, results were promising. However, they were unable to prove non-inferiority as a whole of the tissue preserved for a longer time. To prove this, the confidence interval needed to be 4% or lower, but this was at 5.4%, Dr. Lass reported. However, the overall success rate was high in both groups at around 95% for the tissue preserved for the short time period and 92% for that in the longer preservation group. However, when the subgroup analysis was considered, it became clear that the failures in the longer preservation group were mainly coming from the oldest 12- to 14-day tissue. “In the paper we came out saying that there was no difference up to 11 days, and even at 12 to 14 days, the success rate was at 89%, so it’s still good,” Dr. Lass said. Clinically speaking, this means that there is no difference up to 11 days, but if logistically you need to use tissue that has been preserved for 12–14 days, that’s still good. For eye banks, this means more time to research the donors. “It’s going to give them 3–4 more days to evaluate the tissue and distribute it both domestically and internationally, and there will now be hard evidence that this is OK,” Dr. Lass said. Investigators also determined that most of the failures were coming in the first 60 days after surgery. “Primary donor failure was defined as everything went fine at the time of surgery, but postop the cornea never cleared,” he said, adding that in this initial time period there were 22 failures in the group preserved for longer and 11 in the shorter group. Investigators think that while this tissue may still appear good when considered with the normal process of donor evaluation, it doesn’t withstand the stress of the longest preservation time and fails early on. “There’s a subset, which we can’t detect with our current methods for donor evaluation, that could not withstand that stress,” Dr. Lass said. A separate analysis of cell loss led by Dr. Lass likewise boded well for tissue preserved for longer periods.2 At the 3-year mark, investigators found that this was comparable in the 0- to 7-day preservation group and the 8- to 14-day one. “But again, we found that the longest group had more cell loss of clear grafts in 3 years than the shorter group did,” Dr. Lass said, adding that there was 37% cell loss compared to baseline for the shorter group versus a 40% loss in the longer group. Once again, when a subgroup analysis was done, it was determined that most of the cell loss was coming in that longest preservation group, particularly at day 14. “Again, this supported the findings that it was fine to go out 11 to 12 days,” he said. “It suggests that the preservation time had an effect on the ones that are surviving at 3 years.” This means that it may be necessary to follow these eyes a little longer in order to determine if there are going to be any more late failures in the ones that were preserved for 13 or 14 days. Dr. Lass hopes that practitioners come away from this with a new confidence in using donor corneas that have been preserved for up to 11 days. “There’s no difference,” he said. The hope is to change people’s minds and increase the average preservation time in the U.S. from 7–8 days and move it more toward 10–11 days. “This is going to help eye banks now and in the future as the demand for corneas is going to increase with an aging population,” Dr. Lass said.
References
1. Rosenwasser GO, et al. Effect of cornea preservation time on success of Descemet stripping automated endothelial keratoplasty: a randomized clinical trial. JAMA Ophthalmology. 2017;135:1401–1409. 2. Lass JH, et al. Corneal endothelial cell loss 3 years after successful Descemet stripping automated endothelial keratoplasty in the Cornea Preservation Time Study: a randomized clinical trial. JAMA Ophthalmology. 2017;135:1394–1400. Editors’ note: Dr. Lass has no financial interests related to his comments. Contact information Lass: Jonathan.Lass@UHhospital.org
↧
Research highlight: New benefit of cataract surgery
by Maxine Lipner EyeWorld Senior Contributing Writer

Illustration showing a normal eye and an eye effected with a cataract
How the procedure may impact mortality risk
New study results indicate that cataract surgery can lead to longer life in women. The study published in JAMA Ophthalmology1 indicates that cataract removal in older women is associated with a 60% lower risk of death, according to Victoria Tseng, MD, PhD, resident in ophthalmology, University of California, Los Angeles.
This study was an outgrowth of an earlier investigation, the Women’s Health Initiative. “The original purpose of that trial was to study the effects of hormone therapy and dietary changes in postmenopausal women to see what kinds of outcomes they had,” Dr. Tseng said. “That study was cut short because they found that hormone therapy could be associated with an increased risk of a vascular event.” Even though the trial was stopped early, investigators continued to collect data until 2015, which meant there was 20 years of continuous information on them.
Mortality risk
In the recent study, investigators included only women who had a diagnosis of cataract. “Our goal was to compare people with cataracts who were not operated on and people who had cataract surgery,” Dr. Tseng said, adding that the study population included approximately 73,000 women who had a diagnosis code for a cataract and who were 65 years or older. “We followed them to see how many of them died over time,” she said. “We looked at all-cause mortality and cause-specific mortality.” Investigators grouped the cause-specific mortality into cardiovascular, cancer-related, neurological, pulmonary, infectious, and accidental causes.
“We found that cataract surgery was associated with a decreased risk of not only all-cause mortality but every other kind of mortality for the people who underwent cataract surgery versus those who had a cataract and didn’t get surgery,” Dr. Tseng said, adding that she was surprised that regardless of what kind of mortality they considered here, there was a protective association to cataract removal. Those who underwent the cataract surgery were a little sicker than those who decided not to undergo the procedure, Dr. Tseng noted. The reason for this, however, was unclear.
Anne Coleman, MD, PhD, Fran and Ray Stark Foundation Professor of Ophthalmology, Stein Eye Institute, and professor of epidemiology, Fielding School of Public Health, UCLA, views the fact that mortality was decreased by cataract removal as making sense. “As an ophthalmologist, I was not surprised because I think that people take their vision for granted, and vision helps with functioning in life,” Dr. Coleman said. “If you can’t see, you can’t take your medication—you can mix up your pills because you can’t tell the difference in colors.”
Even walking can become out of the question because of an increased risk of falling. “That limits the amount of exercise you can do because if you’re having trouble seeing, you’re not going to feel comfortable going outside and walking in the park or taking a hike, so people start curtailing their exercise,” Dr. Coleman said. In addition, if you can’t see, you can’t drive and that leads to isolation, which is bad for older individuals who need the social interaction. “When you take out patients’ cataracts, it’s transformative for them,” she said. “The next day, they can see colors, they can read the paper, they can move around easily, and it changes their lives,” Dr. Coleman said. “As a clinician, I think it’s one of the best surgeries you can do.” Transformative surgery
Unfortunately, most ophthalmologists don’t see those who decline to undergo the procedure. “That’s why these types of studies are important because as clinicians we get biased samples of who comes to us,” Dr. Coleman said. She views the information from this study as important to get the word out to primary care doctors and family members to get patients to have their eyes checked for cataracts. Dr. Coleman recalled a patient from the beginning of her career who had count fingers hand motion vision due to cataract and had stage 4 breast cancer. “The internist said it would be worth it to operate on her because she had another 6–12 months to live and it would be ‘transformative,’ and he was right.” After having her cataracts removed, the patient was able to regain some of her own autonomy, and she could see her children and grandchildren. “It was life changing for her,” Dr. Coleman said. Dr. Tseng said that clinically speaking this puts cataract surgery in a new perspective. “Often when someone is ill or there are a lot of things going on, the eyes tend to get neglected,” Dr. Tseng said. “I think you shouldn’t forget about someone’s visual function even if they’re very ill because based on our results, there may be benefits for these patients even if you don’t think that they’re going to live long.” Overall, Dr. Coleman hopes that practitioners remember how important vision is to the overall quality and length of life for patients. “I think we get so focused on our own field that we forget how important vision is,” Dr. Coleman said. “It’s not just for someone’s quality of life but also the length of their life, and it plays an important role in their health.” Ophthalmologists can use this information in talking with other medical colleagues and help educate them, she concluded.
Reference 1. Tseng VL, et al. Association of cataract surgery with mortality in older women: findings from the Women’s Health Initiative. JAMA Ophthalmol. 2018;136:3–10.
Editors’ note: Dr. Coleman and Dr. Tseng have no financial interests related to their comments.
Contact information
Coleman: coleman@jsei.ucla.edu Tseng: vtseng120@gmail.com
Source: https://www.eyeworld.org/new-benefit-cataract-surgery
↧
Tecfen Medical Post Op Cataract and Refractive Kits
Dear Tecfen Customers and Friends,
Did you know we also offer Post-Operation Sunglasses, Eye shields and Kits?
In addition to our wide range of surgical products, we offer a variety of solutions for your post-surgical needs. You can choose from our popular offerings or custom build a kit that best suits your practice.
Below is our most popular Post-Cataract and Post-Refractive kit.
If needed, we can also provide the individual products as well.

TE-671X Economy Post Cataract Kit
– SolarShield Sunglasses
– Single Clear Eye Shield
– Transpore Tape
– Packed in a plastic drawstring bag

TE-672K Premium Post Refractive Kit
– SolarComfort Sunglasses
– Dual Eye Shield
– Packed in a navy blue nylon bag
We are happy to assist you with all your Post-Op requirements. Please contact us for more information and pricing.
↧
↧
Tecfen Medical Trephines are now CE Marked!
Dear Tecfen Customers and Friends,
We are happy to announce that our entire range of Corneal Trephine Products are now CE marked!
This includes our Traditional Trephines, Non-Vacuum Punches, Radial Vacuum Trephines, and Vacuum Trephine Punches.

Our Tecfen Trephines and Punches come in a wide range of sizes. We have eye bank sizes available as well, please inquire.
Please click here to see our entire range of Tecfen Trephines.

Don’t forget to download our current Ophthalmic Catalog where you can see our full range of products.
If you are interested in pricing, please contact us
We will be exhibiting at ESCRS Vienna (21st – 25th September). Please visit our booth B512 or contact us to schedule a meeting.
With over 30 years of experience in the medical industry, Tecfen Medical strives to provide our customers with the highest quality products available to over 100 countries worldwide.
If you have any questions or would like more information, please email us or call us anytime.
Best regards,
Kerim Ekonomi
Vice President
↧
Come see Tecfen Medical at ESCRS Vienna at Booth B512
Dear Tecfen Customers and Friends,
It is that time of year again! We will be exhibiting our Ophthalmic Products at ESCRS Vienna Austria, September 21st – 25th.
Our booth number is B512.

Please stop by to see our entire range of products including our Ophthalmic Knives, Microkeratome Blades, PVA Eye Spears, Trephines (including our Radial Vacuum Trephine and Vacuum Punch), Tano Polishers, Punctum Plugs, and more!
We will also have our popular line of Post-Surgical products on display, including our Post-Cataract/Post-Refractive Sunglasses, Eyeshields, and Post-Op Kits.
If you are interested in arranging a meeting at the conference, please contact us.
We wish you safe travels and look forward to seeing you there!
Best regards,
Kerim Ekonomi
Vice President
↧
Come See us at AAO Chicago at Booth 2050!
Dear Tecfen Customers and Friends,
We will be exhibiting our Ophthalmic Products at AAO Congress in Chicago (27th – 30th October) and we hope to see you there!
Our booth number is 2050.
Please stop by to see our brand new Tano Polishers and Punctum Plugs, as well as our entire range of products. This includes our Ophthalmic Knives, Microkeratome Blades, PVA Eye Spears, Trephines (including our Radial Vacuum Trephine and Vacuum Punch) and more!
We will also have our popular line of Post-Surgical products on display, including our Post-Cataract/Post-Refractive Sunglasses, Eyeshields, and Post-Op Kits.
If you would like to order Tecfen products to be delivered to your hotel, please contact us as soon as possible.
We wish you safe travels and look forward to seeing you there!
↧
The cleanest and most absorbent PVA spears on the market.
Tecfen Medical PVA Spears are one of the cleanest and most absorbent ophthalmic sponges on the market. Have you tried them?
If not, please contact us for samples.
Our range of PVA Spears, Cellulose Spears, Instrument Wipes, and Corneal Light Shields products are precision made in the USA using the highest quality materials.

Please click here to see our full line of PVA products on our website.
Don’t forget to download our current Ophthalmic Catalog where you can see our full range of surgical and post op products.
With over 30 years of experience in the medical industry, Tecfen Medical strives to provide our customers with the highest quality products available in over 100 countries worldwide.
If you have any questions or would like more information, please email us or call us anytime.
Best regards,
Kerim Ekonomi
Vice President
↧
↧
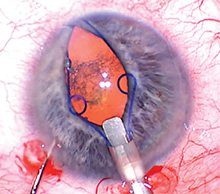
Device Focus Pupil dilating devices Pharmacological vs. mechanical
by Rich Daly EyeWorld Contributing Writer
Amid the proliferation of pupil dilating devices, it remains important to know when cataract patients are best served by them or pharmacological options. If the patient’s pupil dilated well in the preop visit but does not seem as dilated on the operating table, Bonnie Henderson, MD, augments the topical dilation drops with intracameral epinephrine. “The preservative-free epinephrine can be drawn directly from the vial and diluted 1:4 with balanced salt solution and injected into the anterior chamber,” Dr. Henderson said. “I only inject a small amount—about 0.3 cc—turn off the microscope, and allow it to work for 1 minute before continuing the case.” The injection of epinephrine follows injection of preservative-free lidocaine into the anterior chamber. “I have found that epinephrine alone works well and does not seem to cause any discomfort to the patient,” Dr. Henderson said.
If the pupil does not dilate well in the clinic, Dr. Henderson will plan to use a device. “However, if the pupil dilated sufficiently but the patient is on a medication that can cause floppy iris syndrome, I will have the device ready in the operating room,” Dr. Henderson said.
Richard Tipperman, MD, tries adjuvant pharmacological substances for small pupil cases and uses them prophylactically in all femtosecond cases. Additionally, surgeons at Wills Eye Institute use epi-Shugarcaine solution (epinephrine and lidocaine in fortified balanced salt solution) to enlarge pupils during cataract surgery. Mechanical devices Dr. Henderson turns to a mechanical device to help with pupil dilation and maintenance in other circumstances. In the preop evaluation in the clinic, Dr. Henderson evaluates the level of pupillary dilation. She also notes any medications the patient is taking that might affect the pupil. If the pupil does not dilate well in the clinic, Dr. Henderson will plan to use a device. “However, if the pupil dilated sufficiently but the patient is on a medication that can cause floppy iris syndrome, I will have the device ready in the operating room,” Dr. Henderson said. If the iris seems floppy at the beginning of surgery—even after the injection of intracameral lidocaine or viscoelastic—she implants a pupillary dilation device before creating the capsulorhexis. “If the capsulorhexis is already made and the pupil starts to constrict, it is still possible to use hooks or a ring at that time,” Dr. Henderson said. “However, great care must be taken to avoid capturing the edge of the capsule while attempting to capture just the edge of the pupil.” Dr. Tipperman said a poorly dilating pupil clearly is the leading indication in such situations but noted that there are additional considerations as well. “I’m more likely to use a mechanical device with a ‘small pupil plus,’ which is a small pupil plus a very dense lens, a small pupil plus pseudoexfoliation, or a small pupil plus a very shallow anterior chamber,” Dr. Tipperman said. Device selection When the pupil alone is the problem, Dr. Henderson prefers a ring type of device. “However, if I suspect that the zonules are also weak, then I prefer hooks so that I can use the hooks to keep the pupil dilated and to support the capsular bag. I like the adaptability of hooks,” Dr. Henderson said. “Also, with hooks, I can choose the location of the placement and can choose how many to use.” Another situation in which Dr. Henderson prefers to use hooks over rings is during scleral fixation of an IOL. “It is sometimes helpful to use a hook to give additional exposure to the area where the haptic is to be fixated,” Dr. Henderson said. Among situations or patient types where Dr. Henderson modifies her use of a device to dilate the pupil is during manual small or large incision cataract surgery when the lens must be prolapsed out of the capsular bag and into the anterior chamber. “This is very difficult to do with any type of pupillary dilation device in place,” Dr. Henderson said. “Therefore, in these cases, I recommend using a dilation device (either hooks or rings) to dilate the pupil in order to perform the capsule opening and remove the device before prolapsing the nucleus.” Another situation where a surgeon should take caution with pupillary dilation is in cases of patients with uveitis. “In some patients, the iris can become damaged or remain dilated if the iris is stretched with a dilation device,” Dr. Henderson said. “The device may be necessary to perform the surgery safely so it is still prudent to use one, but the surgeon should be aware that the pupil may not constrict back to the same preoperative size.” Dr. Tipperman also has tried multiple devices, but he prefers the Malyugin ring for dilation due to its ease of insertion, placement, and removal. However, Dr. Tipperman avoids the use of the ring in very small pupils or fibrotic pupils, where it can still produce sphincter tears. “Especially if I’m using a multifocal IOL in these cases, I try to avoid mechanical pupillary dilation,” Dr. Tipperman said.
About the doctors Bonnie Henderson, MD Clinical professor Tufts University School of Medicine Boston Richard Tipperman, MD Attending surgeon Wills Eye Hospital Philadelphia Financial interests Henderson
Contact information
Henderson: bahenderson@eyeboston.com
Tipperman: rtipperman@mindspring.com
Source: https://www.eyeworld.org/
↧
The Launch of two NEW Tecfen Medical Products
We are excited to announce the launch of two NEW Tecfen Medical products.
Laser Probes
Compatible with Alcon, Iridex, Coherent, Zeiss, Ellex, Quantel and DORC lasers.
Smooth extension and retraction of curve.
Uniform spot size when straight or curved.
Consistent laser uptake
Direct access to posterior pole
Fixed flexible curve allows easy access through rigid cannula
Smooth transition at taper
*Available in Straight, Curved, Adjustable, and Flexible

Laser Probes
Compatible with Alcon, Iridex, Coherent, Zeiss, Ellex, Quantel and DORC lasers.
Membrane Polishers.
Black silicone tip maximizes the contrast against the retina
Used for neuroepithelial membrane polishing during retinal surgery
Diamond dust ensures the least amount of shed partials in the eye
*Available in 23G and 25G

Head to http://tecfenmedical.com/ophthalmic-surgical-products/ to read more
↧
Tecfen Medical Appoints John Weiss as UK Distributor
Tecfen Medical is now listed as a “Trusted Brand” for John Weiss in the UK.
Tecfen Medical is pleased to announce the appointment of John Weiss as UK distributor of the Tecfen Medical portfolio of corneal trephine blades & tissue punches.
From the Winter issue of the HS-UK/John Weiss ‘InFocus’ newsletter:
John Weiss appointed UK distributor of the Tecfen Medical portfolio of corneal trephine blades & tissue punches.
Tecfen Medical offers a comprehensive selection of corneal trephine blades and tissue punches.
John Weiss is an authorised distributor for the Tecfen portfolio in the UK.
Long Trephine Blades (for donor or recipient) can be used by hand or with a hand piece, such as the Tecfen Corneal Punch system, and are compatible with most punch systems. They deliver consistent results and range from 4 – 18mm in diameter.
Vacuum and Non-vacuum Trephine Punches (for donor) are available as a complete system, with blades ranging from 6mm – 9.5mm in diameter.
Non-Vacuum Trephine Punches are designed with four posts to ensure proper alignment between the punch base and the trephine blade holder, ensuring a perfect cut, every time.
The Radial Vacuum Trephine (for recipient) is a complete vacuum trephine system, with 16 vacuum chambers to provide stability for a clean and precise cut.
For further information on the Tecfen range of corneal trephine and tissue punches, please visit https://jweiss.co/tecfen, or email tecfen@johnweiss.com.
Read the full newsletter here.
↧
Tecfen Medical’s Response to Coronavirus (COVID-19)
Tecfen Medical’s Response to Coronavirus (COVID-19)
As a leading supplier of ophthalmic surgical disposables and post op products, we take our responsibilities seriously and have been taking steps to proactively prepare for the potential effects of COVID-19.
We have also been receiving questions from customers regarding COVID-19 and would like to take this opportunity to address these questions and provide additional information as available.
Is COVID-19 present in your area?
As of March 13, no cases of COVID-19 have been reported in Santa Barbara, CA. However there have been cases of COVID-19 reported in other areas of California, so we are taking extra precautions and preventative measures.
Is COVID-19 affecting business operations at Tecfen Medical?
Currently COVID-19 is not having a substantial effect on our business operations. Regardless, we are taking steps to sterilize surfaces more frequently and encouraging employees to take extra care in regards to personal hygiene. Certain categories of staff are also being asked to work remotely as a temporary protective measure.
Is your supply chain affected?
We have not received any reports of critical suppliers being directly affected by COVID-19. All Tecfen Medical surgical products are manufactured in the USA, so there is potential for disruption if the situation in the United States worsens. We will keep customers updated with information regarding any delays or shortages, and are working with critical suppliers to ensure adequate stock levels. We have recently increased inventory levels across several categories, including Ophthalmic Knives, Trephines, and PVA Spears, which should provide a buffer in the event of supply chain disruption.
What protocols is Tecfen Medical following?
We are following the latest guidelines published by the CDC found here: https://www.cdc.gov/coronavirus/2019-ncov/community/organizations/cleaning-disinfection.html
The guidelines cover surface cleaning protocols, personal hygiene recommendations, worker protection, and a variety of other topics relevant to organizational efforts to prevent the spread of COVID-19.
Please let us know any additional questions, and thank you for your support during this challenging situation.
Tecfen Medical
5385 Hollister Avenue, No. 216
Santa Barbara, California 93111 U.S.A.
Telephone: 805 967 1153
Fax: 805 967 1295
Email: tecfen@tecfen.com
↧
↧
Tecfen Medical’s Response to Coronavirus (COVID‐19) – April Update

Based on recent and substantial changes to the Coronavirus in the USA and California specifically, Tecfen Medical would like to update our customers on the current status.
California currently has a shelter in place (quarantine) in effect, which means non-essential employees are encouraged to remain at home.
We have a group of employees operating remotely, in a work from home format, while a core team remains in the office for fulfillment.
As of today, April 22, 2020, our operations and inventory continue without interruption, and our supply chain and other business partners have demonstrated resilience and reliability during a challenging situation.
We are beginning to see increased orders for PPE (personal protective equipment) such as our dual eyeshields, to allow Doctors and other support staff to return to clinics while providing an extra level of precaution. As we all prepare for a return to normal operations, please know that we are stocked and prepared to meet your needs.
Please let us know any questions or concerns, and please let us know if we can help in any way at this time.
Thank you and take care,
Tecfen Medical
5385 Hollister Avenue, No. 216
Santa Barbara, California 93111 U.S.A.
Telephone: 805 967 1153
Fax: 805 967 1295
↧
Reminder to Check Provita Smokehood Expiration Dates
Dear Tecfen Customers and Friends,
For all Provita Smoke Hood owners, please take some time to check the expiration date on those you have in use. There is a four year shelf life on all hoods, and the expiration date can be found labeled on the front of the smokehood package.
The Provita Smoke Hood is a personal escape hood that provides protection from the effects of most toxic smoke fumes, allowing the wearer vital minutes to calmly evacuate a dangerous smoke filled environment. For use in aviation, marine and ground transportation, as well as high rise buildings.
Please let us know if you need to place an order for smoke hoods, or if you have any additional questions.
The post Reminder to Check Provita Smokehood Expiration Dates appeared first on Tecfen Medical.
↧
The long and short of corneal preservation times
by Maxine Lipner EyeWorld Senior Contributing Writer
Studying graft success in tissue that was preserved up to 14 days
The long and short of corneal preservation times
Just how long can corneal tissue be kept and still remain viable for use? Investigators determined that tissue stored for up to 11 days had success rates equal to tissue preserved for a much shorter period, according to Jonathan Lass, MD, Case Western Reserve, University Hospitals Eye Institute, Cleveland.
This study, published in JAMA Ophthalmology, grew out of an earlier donor graft study, with investigators deciding that the issue of cornea preservation would be the next major question with regard to the donor pool.(1)
Bias against long storage
“There was a major prejudice against using tissue beyond 7 or 8 days even though the intermediate storage solution was approved by the FDA to go out to 14 days,” Dr. Lass said. “Also, we were aware that the eye banks, because of this prejudice, were shipping the tissue out of the country and successfully using it internationally,” Dr. Lass said. Surgeons in the U.S. were reluctant to use tissue that had been preserved longer, based mainly on what they had been taught. “They learned to do this in their fellowships, but there was no solid evidence for doing this,” he said. Included in the study were 1,330 eyes, with about an equal distribution between both groups, Dr. Lass noted, adding that they chose DSAEK as the procedure with which to test preservation time because this is currently the most common keratoplasty technique in use. In this masked study, the only thing surgeons knew about the donor was the thickness of the corneal tissue after lamellar dissection. “They needed that information for doing the procedure,” Dr. Lass said. When a cornea was found to be eligible, this was then assigned to a patient, with half of the individuals receiving corneas that had been preserved for 7 days or less and the other half preserved for 8–14 days. In addition, the groups were subdivided into 0–4 days, 5–7 days, 8–11 days, and 12–14 days.
Considering findings
At the 3-year mark, results were promising. However, they were unable to prove non-inferiority as a whole of the tissue preserved for a longer time. To prove this, the confidence interval needed to be 4% or lower, but this was at 5.4%, Dr. Lass reported. However, the overall success rate was high in both groups at around 95% for the tissue preserved for the short time period and 92% for that in the longer preservation group. However, when the subgroup analysis was considered, it became clear that the failures in the longer preservation group were mainly coming from the oldest 12- to 14-day tissue. “In the paper we came out saying that there was no difference up to 11 days, and even at 12 to 14 days, the success rate was at 89%, so it’s still good,” Dr. Lass said. Clinically speaking, this means that there is no difference up to 11 days, but if logistically you need to use tissue that has been preserved for 12–14 days, that’s still good. For eye banks, this means more time to research the donors. “It’s going to give them 3–4 more days to evaluate the tissue and distribute it both domestically and internationally, and there will now be hard evidence that this is OK,” Dr. Lass said. Investigators also determined that most of the failures were coming in the first 60 days after surgery. “Primary donor failure was defined as everything went fine at the time of surgery, but postop the cornea never cleared,” he said, adding that in this initial time period there were 22 failures in the group preserved for longer and 11 in the shorter group. Investigators think that while this tissue may still appear good when considered with the normal process of donor evaluation, it doesn’t withstand the stress of the longest preservation time and fails early on. “There’s a subset, which we can’t detect with our current methods for donor evaluation, that could not withstand that stress,” Dr. Lass said. A separate analysis of cell loss led by Dr. Lass likewise boded well for tissue preserved for longer periods.2 At the 3-year mark, investigators found that this was comparable in the 0- to 7-day preservation group and the 8- to 14-day one. “But again, we found that the longest group had more cell loss of clear grafts in 3 years than the shorter group did,” Dr. Lass said, adding that there was 37% cell loss compared to baseline for the shorter group versus a 40% loss in the longer group. Once again, when a subgroup analysis was done, it was determined that most of the cell loss was coming in that longest preservation group, particularly at day 14. “Again, this supported the findings that it was fine to go out 11 to 12 days,” he said. “It suggests that the preservation time had an effect on the ones that are surviving at 3 years.” This means that it may be necessary to follow these eyes a little longer in order to determine if there are going to be any more late failures in the ones that were preserved for 13 or 14 days. Dr. Lass hopes that practitioners come away from this with a new confidence in using donor corneas that have been preserved for up to 11 days. “There’s no difference,” he said. The hope is to change people’s minds and increase the average preservation time in the U.S. from 7–8 days and move it more toward 10–11 days. “This is going to help eye banks now and in the future as the demand for corneas is going to increase with an aging population,” Dr. Lass said.
References
1. Rosenwasser GO, et al. Effect of cornea preservation time on success of Descemet stripping automated endothelial keratoplasty: a randomized clinical trial. JAMA Ophthalmology. 2017;135:1401–1409. 2. Lass JH, et al. Corneal endothelial cell loss 3 years after successful Descemet stripping automated endothelial keratoplasty in the Cornea Preservation Time Study: a randomized clinical trial. JAMA Ophthalmology. 2017;135:1394–1400. Editors’ note: Dr. Lass has no financial interests related to his comments. Contact information Lass: Jonathan.Lass@UHhospital.org
The post The long and short of corneal preservation times appeared first on Tecfen Medical.
↧